Excerpt from Michael Flomenhaft’s presentation, given at Zwanger-Pesiri Radiology and Long Island Spine Care Affiliates (LISCA) Symposium, November 16, 2021. He addresses the importance of evaluating white matter injuries.
“Challenges in Proving Long Term Effect of Concussion/ Mild Traumatic Brain Injury”
The biggest source of difficulty and misdirection for attorneys handling concussion cases is failure to recognize that vast percentage of concussions especially in mva’s (motor vehicle accidents) are essentially white matter injuries. White matter refers to the brain’s connectivity which enables brain cells (neurons) to communicate. Yet, physicians who are evaluating these injuries are essentially grey matter doctors. Grey matter represents the brain’s approximately 100 billion neurons that perform the brain’s thinking and processing.
However, most mTBI’s (mild traumatic brain injuries)/concussions whether from mva’s or blast or even falls, are consequences of sudden acceleration/deceleration or whiplash type injuries. It is the white matter injury described as “shearing” from these events which is the dominant mechanism of injury in concussion/ mTBI. Shearing refers to pulling and disturbance of the white matter and its eventual resultant deterioration with an accompanying decline in brain functioning. Because these connections are so delicate and fragile, even low impact mva’s can produce sufficient forces to inflict significant and permanent shearing damage.
Unfortunately, grey matter is what the medical exam is geared to assess; that is what the CT and MRI imaging are sensitive to reliably visualize; and grey matter is the focus of brain neurology education and training for most doctors.
Grey matter lesions have a different presentation and evolution than white matter injuries. Their symptoms and signs are much more obvious from the outset. If present, they can be detected by a Cat Scan from the visualization of hematomas and brain shifting. In contrast, the trajectory of evidence of white matter injury and its manifestations is much more extended and its existence far more difficult to discern on imaging and on clinical examination.
It can often take many hours, days, and even weeks or months for the full cascade of effects of shearing of white matter to appear and be discerned. Obviously, this will often be long after a patient is discharged from the ER. The full functional effects of white matter shearing can develop over time with the emergence of an increasing constellation of cognitive deficits in higher level mental functioning such as reasoning, organization, processing speed, multi-track thinking to name a few which a physician’s mental status exam is not geared to assess.
Because white matter damage is often not as initially highly symptomatic compared to grey matter injury and its effect is on higher level functioning rather than the much more obvious basic mental functioning that physicians are concerned with, the seriousness of this injury is not usually obvious by talking to a patient. It will often take a while, often many months sometimes years for friends and family to observe or grasp the full extent of these changes. Although the person may look and sound the same, it will take time for the serious but nonetheless often subtle and frequently disabling changes in functioning to become cumulatively evident to the point where they become clear.
Complicating the recognition of these changes from concussion, is that the white matter damage associated with concussion described as Traumatic Axonal Injury (TAI) (distinct from Diffuse Axonal Injury) usually has little effect either on intelligence which is quite resilient to concussion trauma or how people speak. Most people equate brain health with intelligence and gauge intelligence by how people speak. If they sound good, then they are good.
In contrast, the cognitive damage that develops in these victims over time is typically not to intelligence, but rather to the ability to use their intelligence. Highly level cognitive abilities such as short-term memory, speed of processing, organization, attention are extremely vulnerable to concussion. These things are not intelligence per se but are crucial to using intelligence effectively. To put it more bluntly: They can talk the talk; but they can’t walk the walk.
For example: An air traffic controller needs multitrack thinking (keeping several things in mind simultaneously) and good mental processing speed (thinking rapidly). These are also examples of higher-level functioning. So while his intelligence may be intact after a concussion, and he may sound fine in conversation, when he sits down at the console, because he has lost his ability to keep track of several flights simultaneously and think quickly enough, those multiple flights he is guiding are at heightened risk for a mishap or crash.
Imaging is Important in Evaluating White Matter Abnormalities
Imaging, typically post trauma imaging CT and MRI do not have the resolution to detect most white matter injury associated with mTBI. MRI visualizes in millimeters (mm); while the diameter of white matter is less than a micron which is one 1/1000 of a mm. To the extent any white matter abnormalities are detected in the form of hyperintensities (white spots on the MRI), they are often incorrectly ascribed solely to cerebrovascular abnormalities as most neuroradiologists are not trained to be concerned with recognition of subtle or non-extreme white matter injury on MRI.
Overtime, white matter injury can eventually cause grey matter atrophy defined as volume loss. However, this can take up to a year, hence the need for more than one MRI to capture and visualize such loss. Quantification technology can assist in demonstrating that volume loss even more accurately.
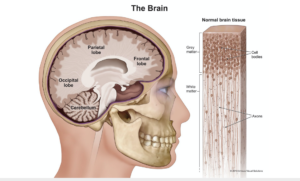
Diagram shows distribution of grey matter and white matter